
Emergency Medical Services (EMS) in Cheyenne County have experienced several ownership and operational transitions over the past few years.
Regional West Medical Services operated EMS services in Cheyenne County from the summer of 2002 through June 2023. When Regional West ended its service, Morrill County Community Hospital stepped in to continue providing emergency medical services to county residents. However, due to increasing operational costs, Morrill County Community Hospital discontinued the service in September 2024.
To prevent disruption in emergency medical care, Sidney Regional Medical Center, the City of Sidney, and Cheyenne County partnered to establish a new EMS organization for Cheyenne County. While this collaboration successfully maintained ambulance service for the community, the funding model originally established is no longer sufficient to cover current operating expenses.
Several factors have contributed to the financial challenges facing EMS today:
Rising Costs Due to Inflation
Since 2018, cumulative inflation has increased by 32.56%, according to the U.S. Bureau of Labor Statistics. The impact is evident across EMS operations. For example, the purchase price of a new ambulance is now approximately $350,000, $100,000 higher than it was prior to the COVID-19 pandemic. It now costs about $100,000 to stock an ambulance for ALS services. The State of Nebraska has deemed Fire Rescue, Law Enforcement, and Emergency Medical Services essential service in communities. EMS was not specifically given a funding mechanism, meaning there is no established method of paying for the EMS service.
Increased Demand for Service
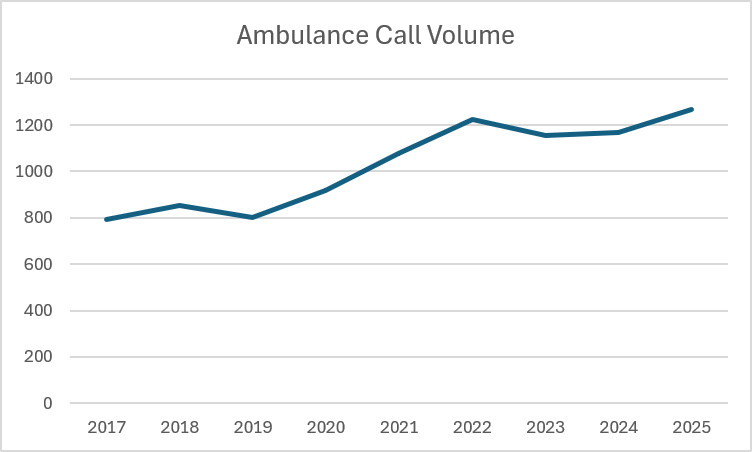
The demand for ambulance services in Cheyenne County has increased significantly. Between 2017 and 2025, EMS call volume increased by 37.6%, requiring additional staffing, equipment, and operational resources. With the increase in call volume, Cheyenne County has seen an increase in median age since 2018. In 2018 the median age was 40.7 and in 2025 it was 42.5. The percentage of the population, 65+, has also risen from 22.7% to 23.3%.
| SRMC EMS Response Type Jan 26 – May 26 | ||
|---|---|---|
| Response Type of Service Requested | # of Runs | % of Total Runs |
| Emergency Response (Primary Response Area) | 405 | 81.82% |
| Hospital-to-Hospital Transfer | 50 | 10.10% |
| Emergency Response (Intercept) | 9 | 1.82% |
| Standby | 7 | 1.41% |
| Support Services | 24 | 4.85% |
Changes in Insurance Coverage and Reimbursement
The mix of insurance coverage among Cheyenne County residents has shifted substantially since 2018. EMS agencies typically receive lower reimbursement rates from government-funded programs and uninsured patients than from employer-sponsored insurance plans. Since September of 2024 non-employer insurance has made up 62% of the calls.
| Insurance Type | Year | Percentage of Population |
|---|---|---|
| Employer Ins. | 2018 | 56.10% |
| Employer Ins. | 2024 | 42.90% |
| Non-Group | 2018 | 11.90% |
| Non-Group | 2024 | 18.60% |
| Medicare | 2018 | 12% |
| Medicare | 2024 | 15.80% |
| Medicaid | 2018 | 11.00% |
| Medicaid | 2024 | 14.60% |
| Uninsured | 2018 | 7.34% |
| Uninsured | 2024 | 6.78% |
Datausa.io/profile/geo/Cheyenne-county-ne
The percentage of residents covered by employer-sponsored insurance has declined by more than 13 percentage points, while enrollment in Medicare and Medicaid has increased. These changes place additional financial pressure on EMS operations because reimbursement rates never cover the cost of providing emergency medical services. The average reimbursement on billed services for EMS has been 32%.
As costs continue to rise and service demand increases, Cheyenne County faces the challenge of identifying a sustainable funding solution that will ensure reliable emergency medical services for residents now and into the future.
How EMS Works: Understanding Volunteer and Paid Emergency Medical Services
Emergency Medical Services (EMS) is the system of pre-hospital care that responds to medical emergencies in our communities. When someone calls 911, the type of EMS system serving that area, volunteer, paid, or a combination, shapes how quickly help arrives and what level of care is provided.
What Is EMS?
EMS encompasses the personnel, vehicles, equipment, and systems used to respond to medical emergencies before a patient reaches a hospital. This includes situations such as cardiac arrest, stroke, traumatic injury, respiratory distress, and many other medical crises.
- Emergency Medical Technicians (EMTs) deliver foundational assessments, treatment, and patient transport.
- Paramedics provide advanced life support, including cardiac monitoring, advanced airway management, and a wider range of medications and procedures.
| EMS Providers | Course Cost | Time to Acquire | Continuing Education Requirements every 2 years |
|---|---|---|---|
| Emergency Medical Technician (EMT) | $1,200 – $2,000 | 3 – 6 months | 40 hours of Continued Education; Basic Life Support Certification; Driving Courses |
| Paramedic | $8,000 – $13,000 | 3 – 6 months (must have EMT certification first); 1.5 – 2 years; 1 month state examination | 60 hours of Continued Education; Advanced Cardiac Life Support Certification; Pre-hospital Trauma Life Support Certification; Pediatric Advanced Life Support Certification; Basic Life Support Certification; Neonatal Resuscitation Certification; Driving Courses |
All EMS providers operate under physician medical direction and are required to maintain ongoing certifications and continue education to remain licensed.
Volunteer EMS
Volunteer EMS agencies are staffed by individuals who provide emergency medical services without pay. These people usually work full-time jobs elsewhere in the community and may not always be available for calls. Volunteer services offer BLS (Basic Life Support) services since many volunteers are EMTs.
When a call is received, volunteers are paged or notified when a call comes in and respond from wherever they are at the time, home, work, or elsewhere. They travel to a station to retrieve the ambulance before heading to the call site. Response depends entirely on how many volunteers are available and able to respond at that moment.
Volunteer EMS agencies across the United States have experienced significant declines in participation over the past two decades. Medical officials in Nebraska have warned that the state faces a shortage of paramedics and EMTs, particularly in rural communities. The Nebraska Department of Health and Human Services (DHHS) has identified several factors contributing to this trend.
Aging demographics have had a substantial impact on rural areas. Many communities have seen a decline in their younger adult population, reducing the number of individuals available to volunteer. Those who remain must also be willing and able to meet the physical and emotional demands associated with emergency medical services. As a result, the limited number of volunteers often face increased workloads, leading to burnout as communities rely on them to respond consistently to emergencies.
At the same time, the rising median age in rural communities has increased the demand for EMS services, resulting in higher call volumes and placing additional strain on already limited volunteer resources. Economic pressures have further compounded the problem. Inflation and rising living costs have forced many individuals to work multiple jobs, leaving less time available for volunteer service.
Additional challenges include changing work schedules, longer commuting distances, the prevalence of dual-income households, and the significant time and financial commitments required for EMT training and certification. Together, these factors have contributed to the ongoing decline in volunteer EMS participation and have created significant staffing challenges for rural emergency medical services.
Volunteer providers must meet the same state certification standards as paid providers. Becoming an EMT requires approximately 120-150 hours of training; paramedic certification requires significantly more. Maintaining certification requires ongoing continuing education. This has resulted in many of the volunteer services mainly running on EMTs and being shorthanded with paramedics. The cost and time commitment usually push paramedics to a full-time agency where they get paid.
Because volunteer response depends on who is available to respond at the time of a call, response times can vary considerably. In the Western Nebraska region, data shows the average time from dispatch to a unit being enroute is 19 minutes and 47 seconds for volunteer services, and the average total response time, from call received to arrival on scene, is 49 minutes and 2 seconds.
It is also worth noting that in a volunteer system, there is no requirement that any individual volunteer must respond to a given call. If too few volunteers are available to respond, mutual aid from another agency may be needed, which can extend response times further.
Paid EMS
Paid EMS services employ career professionals who work scheduled shifts and are stationed at a facility during their duty hours, ready to respond immediately when a call comes in. Paid crews are on duty at a station or in the ambulance. When dispatched, they respond directly from that location without needing to travel from home or another location first. Staffing is scheduled in advance to ensure coverage at all hours.
Because staffing is based on scheduled shifts rather than voluntary availability, paid EMS services provide consistent coverage regardless of time of day, day of week, or other factors. Nights, weekends, and holidays are staffed the same as any other time.
SRMC’s average time from dispatch to a unit being enroute is 2 minutes and 40 seconds, and the average total response time is 9 minutes and 46 seconds.
Paid EMS providers meet the same certification requirements as volunteers. Career providers who respond to calls on a full-time basis often accumulate patient care experience more quickly due to higher call volume exposure.
Paid services typically operate under formal quality improvement programs that review patient care data, track performance metrics, and identify areas for ongoing improvement.
Ambulance services typically provide two levels of care based on the licensure and training of their personnel: Basic Life Support (BLS) and Advanced Life Support (ALS). BLS is the most common level of service, particularly among volunteer ambulance organizations, and is provided by Emergency Medical Technicians (EMTs). BLS focuses on immediate patient care and stabilization through interventions such as CPR, rescue breathing, bleeding control, oxygen administration, and the use of an Automated External Defibrillator (AED).
ALS includes all BLS capabilities while providing a higher level of prehospital medical care. ALS services are delivered by paramedics and may include advanced airway management, intravenous (IV) access, medication administration, cardiac monitoring, advanced cardiac life support, and other invasive procedures. Sidney’s current EMS service staffs a paramedic on every shift, ensuring that ALS-level care is available and can be provided when needed during emergency responses.
Why Response Time Matters
Response time is one of the most clinically significant factors in emergency medical care. For time-sensitive conditions, outcomes are directly tied to how quickly treatment begins.
In cardiac arrest, for example, survival rates decrease significantly with each minute that passes without CPR or defibrillation. Guidelines from the American Heart Association recommend defibrillation within minutes of collapse for the best chance of survival. Stroke, severe trauma, and other emergencies similarly have time-dependent treatment windows.
The regional data from Western Nebraska illustrates the difference in response times between the two models:
| Volunteer EMS (Western NE Region Avg.) | SRMC Paid EMS | |
|---|---|---|
| Avg. dispatch to enroute | 19 min 47 sec | 2 min 40 sec |
| Avg. total response time | 49 min 2 sec | 9 min 46 sec |
These figures reflect regional averages and will vary based on geography, call location, staffing levels, and other factors.
Funding EMS Services
Both volunteer and paid EMS systems require financial resources to operate, though the cost structures differ significantly.
While volunteer labor eliminates personnel costs, agencies still incur expenses for vehicles, equipment, fuel, maintenance, training, insurance, communications, and administrative operations. Funding typically comes from a combination of billing for transport services, municipal or county allocations, donations, and fundraising.
Paid EMS costs include:
- Salaries and benefits for full-time personnel
- Vehicles (modern ambulances typically cost $350,000 or more)
- Medical equipment and medications ($100,000 per ambulance)
- Ongoing training and certification
- Facilities, communications, and administrative support
The Importance of Multiple Ambulances
Emergencies Don’t Wait. Neither Can We.
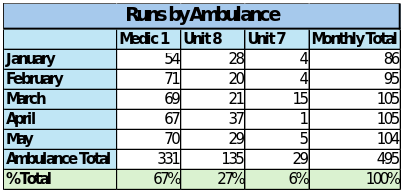
Although Cheyenne County is a rural community, the demand for emergency medical services continues to grow. Sidney EMS responds to an average of approximately 100 calls each month, and there are many situations when more than one ambulance is needed at the same time.
With Interstate 80, Highway 30, and Highway 385 running through our region, we experience a significant number of emergencies. The Nebraska Association of County Officials reports that 21%, or approximately 2,000 residents in Cheyenne County, live outside of towns. The road and country living emergencies can tie up ambulances longer because of the travel time. During the first five months of 2026, Sidney EMS had two ambulances deployed simultaneously 135 times and all three ambulances in service at the same time 29 times. These situations are often the result of patient transfers, serious vehicle accidents, or multiple emergency calls occurring at once.
Recent events, including a gas line explosion and increased concerns about terrorism-related incidents, highlight the importance of maintaining adequate emergency response resources.
There are also occasions when two ambulances respond to the same call. This commonly occurs during lift assists or when additional personnel are needed to safely and quickly load a patient for transport. Sending multiple ambulances helps ensure the highest level of patient care while reducing the need to request assistance from other emergency services.
If only one ambulance were available, there would be times when residents would have to wait longer for emergency medical care. Depending on the circumstances, those delays could be significant. If ambulance services were operated solely by volunteers, response times could increase even further.
Time Is Critical
In emergency medicine, every minute matters. The concept of the “Golden Hour” refers to the first 60 minutes following a traumatic injury, the period that can significantly influence survival, recovery, and long-term outcomes.
The Golden Hour can be viewed in three critical phases:
First 20 Minutes
- An emergency call is made.
- EMS personnel arrive on scene.
- Life-saving care begins.
- The patient is prepared for and transported to the hospital.
Second 20 Minutes
- The patient arrives at the hospital.
- Medical staff conduct assessments and diagnostic testing.
- Treatment plans are developed and initiated.
Final 20 Minutes
- Critical procedures or surgery are performed.
- Medical teams work to stabilize the patient and prevent further complications.
Having multiple ambulances available helps ensure that emergency care begins as quickly as possible, even when several calls occur at the same time. In many situations, those minutes can make the difference between life and death.
Proposed District
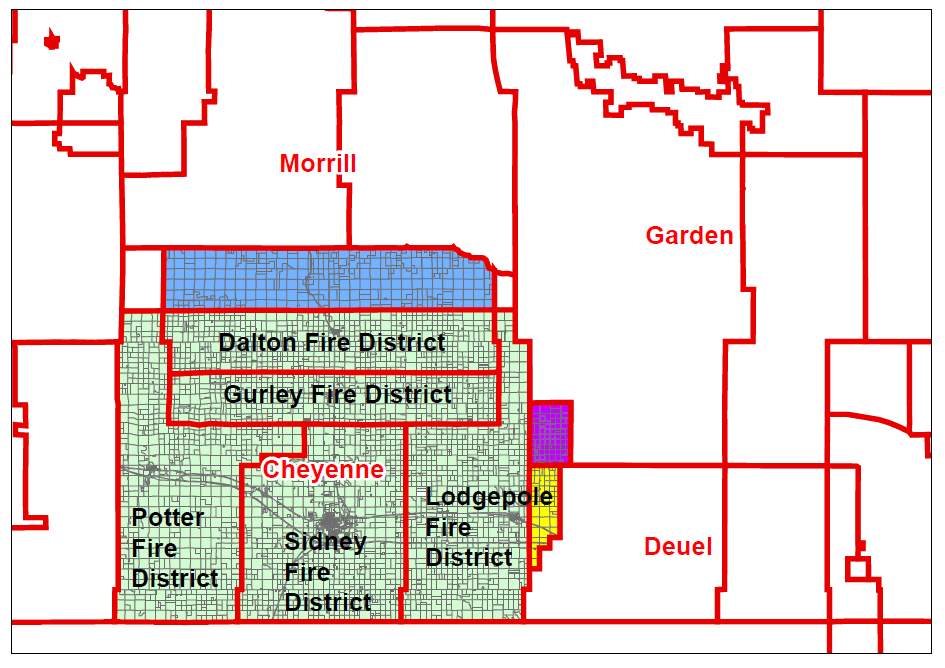
The proposed solution to maintain a full-time Emergency Medical Services (EMS) program in Cheyenne County is the creation of a district known as Western Nebraska Hospital District 1. This will provide stable, long-term funding and oversight into full-time emergency medical services in Cheyenne County. It will mirror the 5 fire districts currently operating in Cheyenne County (Potter Fire District, Dalton/Gurley Fire District, Lodgepole Fire District, Sidney Fire District, and Sidney Rural Fire District).
The district would operate at the county level and be governed by a five-member board. The first board would be appointed by the County Commissioners. After that, the positions would be voted on in an election. They would serve two-year rotating terms. The board would be responsible for overseeing the operations of Western Nebraska Hospital District 1, including obtaining proposals and quotes from EMS providers, contracting services, authorizing payments, and making decisions regarding district operations and services.
Some of the funding for the district would be generated through an increase in the county’s existing levy. This funding structure is intended to provide a stable, long-term source of revenue to help support and maintain EMS services for Cheyenne County residents. Estimated costs for running the current ambulance service provided by SRMC are $1.2 million. The levy increase being proposed is .035 per $100. This would generate approximately $421,262 for the district.
The proposal will be placed on the November ballot for voter consideration.